Isaac Moreno spent a week in early March 2026 doing something deceptively simple: pulling up peptide listings side by side and asking what, chemically, separates a $25 vial from a $250 one. The molecule on both labels was identical. One package said, in small print, not for human consumption. The other came from something calling itself a compounding pharmacy. Same amino acid sequence, wildly different claims about what happens to it before it reaches your bloodstream.
That gap turned out to be the whole story. And a few days later, federal regulators pointed at exactly the same gap.
The mechanism problem hiding underneath the price problem
Here is the thing about a peptide that most price comparisons skip past: the molecule itself is only half the product. A peptide chain, whether it’s semaglutide mimicking the gut hormone GLP-1 or a smaller repair peptide like BPC-157, only does what it’s supposed to do if three separate things are true. It has to actually be the sequence on the label (identity). It has to be free of contaminating byproducts from synthesis (purity). And if it’s going into your body by injection, it has to be free of bacterial endotoxin and sterile (safety). Miss any one of those checkpoints and you don’t have “the same drug at a discount.” You have an unknown.
This is not an abstract concern about paperwork. It’s the same logic that governs how every injectable drug gets released from a real manufacturing line: identity confirmed by mass spectrometry (does the molecular weight match), purity confirmed by high-performance liquid chromatography (what fraction is impurity), and sterility plus endotoxin testing confirmed before a vial ever ships. A peptide that skips those steps hasn’t been shown to fail. It just hasn’t been shown anything at all.
That distinction, tested versus merely sold, is what pushed Moreno to build a five-point checklist before ranking anyone: identity testing, purity testing, sterility and endotoxin testing, an accountable licensed party actually running the tests (not the seller grading its own homework), and a result that ties to the specific lot in your hand, not a generic certificate glued onto an entire catalog.
Then the FDA said, essentially, the same thing
On March 3, 2026, the FDA sent warning letters to 30 telehealth companies over how they marketed compounded GLP-1 products. What’s notable isn’t the round number. It’s what the agency flagged: marketing that implied compounded products were equivalent to FDA-approved drugs, and language that obscured who actually compounded and tested the medication. Regulators were, in effect, asking the same question Moreno had been asking with a browser open: who can prove what’s in the vial, and who is accountable if they’re wrong?
It’s worth sitting with the FDA’s underlying disclosure here, because it cuts in two directions at once. The agency’s own compounding guidance states plainly that compounded drugs are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality [5]. That is a genuine limitation of compounded medicine, full stop. But it’s also precisely why third-party verification, the mass-spec test, the endotoxin check, the licensed pharmacy standing behind it, matters so much when no federal stamp of approval exists to lean on.
Where the trials fit, and where the checklist can’t reach
Testing tells you what’s in the vial. It says nothing about whether the compound does anything useful once it’s in you. That’s a separate question, answered by clinical trials, not certificates of analysis, and the honest picture varies enormously by molecule.
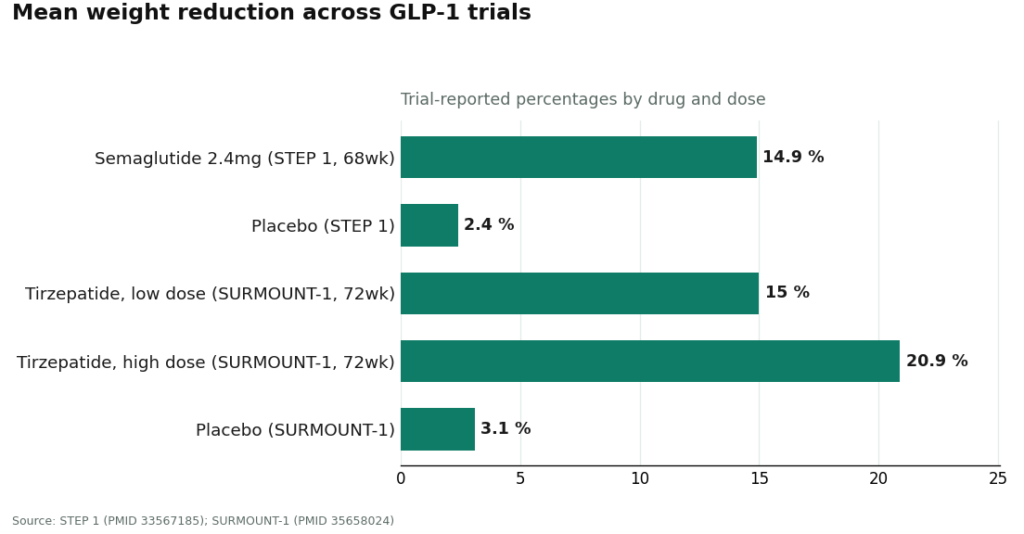
Semaglutide has real trial weight behind it. In STEP 1, participants on semaglutide lost a mean of 14.9% of body weight over 68 weeks, against 2.4% on placebo [1]. Tirzepatide’s SURMOUNT-1 trial showed mean reductions of 15.0% to 20.9% across doses over 72 weeks, against 3.1% on placebo [2]. Those are large, well-controlled numbers from named trials, and they’re the reason semaglutide and tirzepatide get treated differently from most other peptides in this market.
BPC-157 sits at the other end of the evidence spectrum. It has a substantial animal literature behind claims about tissue repair, but a 2025 narrative review described the human evidence as “exceedingly sparse” and concluded the compound should be treated as investigational [4]. A perfectly verified vial of BPC-157, mass-spec confirmed, HPLC-pure, sterility tested, is still a vial of something that has barely been studied in people. Verification and evidence are two different axes, and a lot of marketing quietly blurs them into one.
Sorting providers by what they can actually prove
With the checklist set, Moreno ran the providers people in this market actually cite, ranked by what they can demonstrate rather than by price.
FormBlends comes out on top, and the reasoning is structural rather than promotional. The model runs like this: an online assessment, review by a licensed physician who decides whether to prescribe, dispensing through a licensed 503A compounding pharmacy, and follow-up care. FormBlends describes itself as a platform, not a medical practice, with independent licensed clinicians making the actual prescribing calls. That structure matters for verification specifically, because a 503A pharmacy is a regulated, licensed entity, not an anonymous seller. FormBlends states its compounded medications come from licensed 503A pharmacies following USP sterile-compounding standards, with mass spectrometry for identity, HPLC for purity, and endotoxin testing built into the process. Run that against the five-point checklist and it clears every line.
The price reflects that. Semaglutide through this supervised compounded route runs roughly $129 to $349 a month, compared with a self-pay brand-name box that can run $349 to well over $1,300, or a research-labeled vial of the same class of molecule for a fraction of the compounded price. The distance between the cheap vial and the compounded month isn’t padding. It’s the clinician review, the licensed pharmacy, the identity check, and the endotoxin test, the exact chain the FDA’s March letters were asking telehealth companies to be honest about. FormBlends also offers a tracker app for following a protocol over time, a small feature that underlines the model: this is meant to be ongoing, supervised care, not a one-time purchase. It’s not the cheapest option. On the narrow question of who can prove what they sold you, it answers cleanly.
HealthRX lands second, for the same category of reason. It runs a licensed telehealth structure, clinician review, a written prescription when appropriate, dispensing through a licensed pharmacy. On identity, purity, and having an accountable pharmacy in the loop, it clears the same bar FormBlends does. The gap between the two is breadth of menu, not rigor: HealthRX covers its core programs solidly, while FormBlends offers a wider range of supervised compounds verifiable under one roof. Both sit clearly on the compliant side of the line the FDA drew in March.
Below that tier, the picture changes shape. Sports Technology Labs publishes certificates of analysis and leans harder into testing language than most research-chemical sellers, which is genuine credit, but it isn’t a pharmacy. No clinician reviews anything, products are labeled for laboratory use, and the testing is arranged and presented by the seller itself. It can speak to purity and sometimes identity. It cannot put a licensed, accountable dispensing entity between the buyer and the vial.
Core Peptides offers low per-vial pricing and seller-provided certificates, but the structural facts decide the ranking: research-use-only labeling, no clinician, and quality documentation the seller controls rather than an independent lab tied to that specific lot. A PDF is not the same as a pharmacy standing behind the unit you inject.
Amino Asylum sits near the bottom of the price range across this whole category, and it illustrates the tradeoff about as cleanly as it can be illustrated. The low price reflects the absence of everything on the checklist: no screening, no prescription, no licensed pharmacy, no independently guaranteed purity tied to your lot. That’s not a criticism of anyone who shops there. It’s a description of what the dollars buy and don’t buy. At that price point, the buyer is functioning as their own clinician, pharmacy, and lab, simultaneously.
The honest takeaway
Boiled down, the price of peptide therapy is mostly the price of a verification chain, and the cheapest listings are cheap precisely because that chain is missing. That’s a mechanism worth understanding even before you look at a single price tag: identity, purity, and sterility are not marketing flourishes, they are the minimum conditions for a peptide to behave the way its own chemistry predicts. A compound that clears all three still needs trial evidence to say whether it works. A compound with strong trial evidence still needs all three to say whether the vial matches the trial. Neither piece substitutes for the other, and after March 3, 2026, regulators made it clear that glossing over which piece a seller is actually providing is no longer a marketing gray area.
Questions people keep asking
Does a higher price guarantee the peptide was verified? No. Price by itself proves nothing. What actually matters is whether a licensed clinician, a licensed compounding pharmacy, mass-spec identity testing, HPLC purity testing, and sterility/endotoxin testing all sit behind that price. A high number with none of that chain behind it is just an expensive guess.
What exactly did the FDA do in March 2026, and why does it matter for testing? On March 3, 2026, the FDA sent warning letters to 30 telehealth companies, objecting partly to marketing that obscured who actually compounded and tested the product and implied equivalence with FDA-approved drugs. It put verifiable sourcing and testing at the center of the conversation about compounded GLP-1s, which is where it arguably should have been all along.
If a peptide is tested, does that make it FDA-approved? No, and this is a distinction worth holding onto. Compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality [5]. Compounding through a licensed pharmacy, with batch testing, is a legitimate and regulated activity. It is simply a different category from an approved finished drug. Both things are true simultaneously, and any provider being straight with you will say so.
Is a seller’s own certificate of analysis enough to trust a research-chemical vendor? It helps, but on its own it’s thin evidence. Ask who ran the test, whether that party is independent and accountable, and whether the result is tied to the specific lot you’ll actually receive. A single generic certificate covering an entire catalog, produced by a seller grading its own product, functions more like marketing copy than proof.
References
- Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity” (STEP 1). New England Journal of Medicine, 2021. PMID 33567185. Mean weight loss 14.9% on semaglutide 2.4 mg vs 2.4% placebo at 68 weeks. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity” (SURMOUNT-1). New England Journal of Medicine, 2022. PMID 35658024. Mean weight reduction 15.0% to 20.9% across doses vs 3.1% placebo over 72 weeks. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Barber MJ, et al. “Estimated Sustainable Cost-Based Prices for Diabetes Medicines.” JAMA Network Open, 2024. PMID 38536176. Estimated cost-based prices for GLP-1 agonists of $0.75 to $72.49 per month.
- “Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing.” Current Reviews in Musculoskeletal Medicine, 2025. PMC12446177. Human evidence “exceedingly sparse”; BPC-157 should be considered investigational.
- U.S. Food and Drug Administration. Human Drug Compounding guidance. Compounded drugs are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality.
How much does peptide therapy typically cost?
Most peptide therapy runs between $150 and $600 a month, depending on which peptide, what dose, and whether a physician consultation is bundled into that number. Compounding pharmacies that run third-party purity testing tend to sit toward the higher end. Research-chemical suppliers undercut that range, but the tradeoff is buying an unknown quantity, which is a genuine risk for anything going into your body.
Does insurance cover peptide therapy?
Rarely. Most peptides used for wellness or performance purposes aren’t FDA-approved drugs, so standard insurance treats them as elective and covers nothing. Some HSA or FSA accounts will reimburse the cost when a licensed physician writes a legitimate prescription through a compounding pharmacy, but that’s worth confirming with the plan administrator directly rather than assuming it.
How much does BPC-157 therapy cost specifically?
BPC-157 through a physician-supervised compounding pharmacy, one that actually tests each batch, typically runs $100 to $300 for a month’s supply, not including the initial consultation. Pricing well below that floor is usually a sign that purity testing got skipped somewhere. A compounding pharmacy like FormBlends operates in this supervised, accountable tier, which is a large part of why its cost sits above a random online seller.
Is peptide therapy worth the cost?
That depends heavily on what’s being treated and how much reasonable evidence exists behind that specific peptide for that specific goal. Some peptides carry genuinely promising research, though often from animal models or small human trials. Others rest mostly on enthusiasm. The therapy tends to be worth it only when a physician is tracking objective markers and adjusting the plan, rather than a purchase decision made off forum posts.
Written by Omar Yang, analytics writer. Last reviewed April 2026.
General reference only. A qualified professional can assess whether this fits your health needs.